

Written By: Mikaela Louie
Edited By: Keith Fraga
Despite growing public awareness of its impacts, plastic use continues to have detrimental effects on the environment. Public opinion turning has pushed companies to use biodegradable/compostable packing (i.e., eco-friendly materials) and to invest in new sustainable practices. One recent example is Starbucks’s plan to stop using plastic straws by 2020.
Industry development of biodegradable plastics is also growing, but the types of products available are limited. Additionally, the vague definitions of biodegradable, compostable, and recyclable plastics are not transparent to the public and are often used to “green wash” products that might otherwise continue to have a negative impact. For example, Peak Products has developed biodegradable nitrile gloves. While this is a promising step towards sustainability, it is unclear if these gloves actually degrade faster in landfills than regular nitrile gloves and that the products resulting from their breakdown are indeed better for the environment. As a biology graduate student researcher, I often find my research practices in conflict with my concern for the environment. The need for sterile materials at the lab bench results in prolific use of single-use plastics. Therefore, while many industries work to ban plastic use, most research facilities cannot comply with these changes and are left with few options for alternative materials.
Environmental Impact of Plastic
Plastic waste is mounting in the environment. An estimated 8300 million metric tons (Mt) of plastics have been manufactured to date, resulting in 6300 Mt of plastic waste, the most common being plastic water bottles. Only 9% of this waste is recycled, with 79% of it heading to landfills and the remaining 12% being incinerated. Macroplastics, such as plastic water bottles and disposable utensils, disposed in landfills end up in agricultural land and the ocean as microplastics. Consumption of these microplastics by marine organisms has a severe impact on the marine food chain due to the physiological damage caused by ingestion. Not only are we destroying the surrounding environment, but we are also disrupting the health of our food sources.
The most commonly used plastic for single-use items is polyethylene, and thankfully there is evidence of bacteria and fungi that degrade polyethylene. However, the landfill environment is most likely not conducive for the degradation of such large amounts of waste by a small population of microorganisms.
In an average week (7 days because the cells won’t let me have weekends), I use more single-use plastic than I care to admit. I broke down the amount I use by experiment and type of item:
Cell culture maintenance (one plate)
Volumetric pipette: 14
Glass pipette (not plastic but still trash): 14
Passaging cells (usually 2x a week)
Pipette tip: 16
Volumetric pipette: 12
15mL tube: 4
qPCR (4 different samples, 5 targets)
Pipette tip: 82
1.5mL tube: 10
qPCR plate: 1
Immunohistochemistry on tissue sections
1.5mL tube: 5
Pipette tip: 16
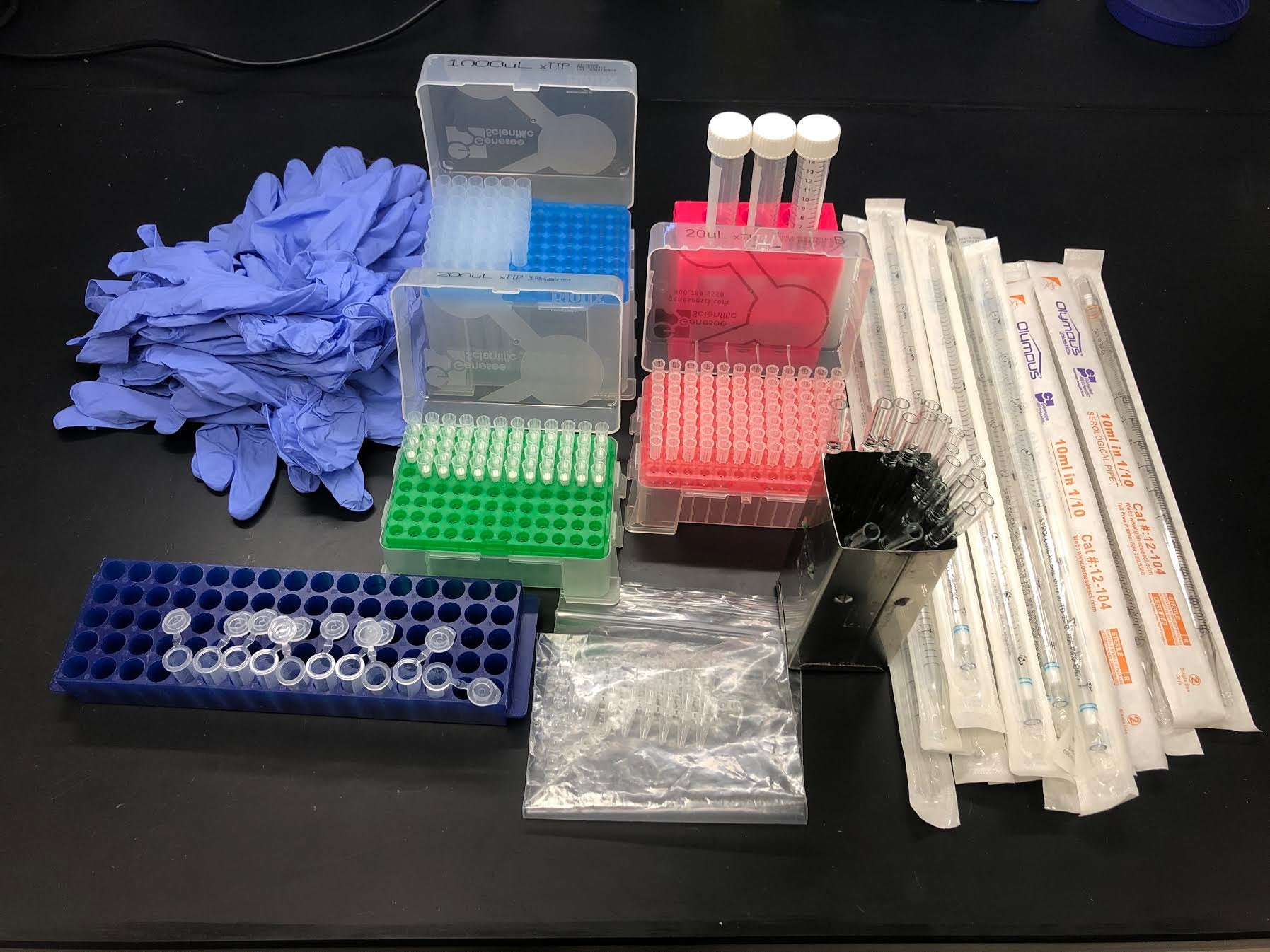
Figure 1: Visual representation of average plastic use in one week.
These averages are also assuming that I don’t make any mistakes, forcing me to throw the item away without actually using it. Even if I made zero mistakes, this amount of plastic from a single week would take thousands of years to degrade. Reflecting on my plastic use and its environmental impact has motivated me to learn what changes are being made and to help align many researchers’ environmental values with their research practices, including my own.
Green Lab Programs
Many universities have begun their own green lab programs, such as MIT and here at UC Davis. Most of these programs evaluate labs on several categories, including energy use, waste production/management and transportation. Labs can participate in these programs to gain certification and to contribute to university wide sustainability practices.
Outside of university-run programs are non-profit groups like My Green Lab. They have created several programs, including a Green Lab certification and the International Laboratory Freezer Challenge. The Freezer Challenge is a competition to see how efficiently labs can store samples and maintain freezers to reduce energy output. The Green Lab website also includes several links to resources for ways labs can implement sustainable practices, such as glove recycling and waste reduction tips. Vendors also have recycling programs for items such as gloves, empty plastic packaging, and pipette boxes. Origin Materials, a UC Davis alumni founded start-up, is also developing biomass polymer products that can supposedly degrade faster than petroleum based plastics. Most of these programs require effort from labs to sort recyclables, and usually only accept items that have no hazardous contaminants. These programs can be established for labs by contacting the local vendor representative.
A Few Takeaways
Single-use plastics are extremely useful. They have allowed science to design well-controlled experiments in an economical way. However, we cannot ignore the consequences that we now face due to our enthusiastic plastic use. It is undeniable that we cannot return to a culture without plastic, but it is becoming more and more necessary to develop plastics that more readily degrade and/or better recycling methods than the ones currently in place. We are also entering a new era of recycling due to China’s refusal of our recyclable waste. This poses an urgent need for better recycling infrastructure within the US. How will this change the ecosystem of materials, packaging, and consumer marketing? Will there be a cultural shift to better recycling practices, such as infrastructure to process difficult-to-recycle materials, and commitment to necessary education for proper recycling practices?
Lessening the amount of plastic that we use is probably the best way that we can reduce our carbon footprint in labs without establishing new programs. This is pretty hard to do with the need for sterility, yet can be accomplished by planning experiments ahead of time and minimizing mistakes. In 2016, UC Davis was named the most sustainable university in the world. Therefore, it seems only fitting that we apply sustainable practices in our research labs as students of UC Davis.
